Natural Treatment For Hammer Toes
 Overview
Overview The term hammertoe describes three unique contracture deformities of the toes. The deformities differ by the location of contracture in each joint of the toe. The three deformities include hammer toe, claw toe and mallet toe. Hammer toes may be flexible or rigid. Hammer toes are most common on the lesser toes (2-5) and may affect one or more toes simultaneously. Hallux malleus is the term used to described a hammer toe of the great toe. Hallux malleus is often found as an isolated foot problem. Hammer toes are found equally in men and women. The onset of hammer toes is between the ages of 30 and 80 years of age.
Causes
It is possible to be born with a hammer toe, however many people develop the deformity later in life. Common causes include tightened tendons that cause the toe to curl downward. Nerve injuries or problems with the spinal cord. Stubbing, jamming or breaking a toe. Having a stroke. Being a diabetic. Having a second toe that is longer than the big toe. Wearing high heels or tight shoes that crowd the toes and don?t allow them to lie flat. Aging.
 Symptoms
Symptoms Common symptoms of hammertoes include pain or irritation of the affected toe when wearing shoes. corns and calluses (a buildup of skin) on the toe, between two toes, or on the ball of the foot. Corns are caused by constant friction against the shoe. They may be soft or hard, depending upon their location. Inflammation, redness, or a burning sensation. Contracture of the toe. In more severe cases of hammertoe, open sores may form.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
If you have hammer toe, avoiding tight shoes and high heels may provide relief. Initial (non-surgical) treatment for hammer toe involves wearing shoes with plenty of room in the toe area. Shoes should be at least one-half inch longer than the longest toe. Stretching and strengthening exercises for the toes (such as picking up items with the toes or stretching the toes by hand) are also recommended. Sometimes orthopedists recommend special pads, cushions, or slings to help relieve the pain of hammer toe.
Surgical Treatment
Hammertoe surgery is performed when conservative measures have been exhausted and pain or deformity still persists. The surgery is performed on an outpatient basis. It typically required about one hammertoe hour of time. An incision is placed over the inter-phalangeal joint. Once the bone is exposed, the end portion of the bone is removed. Your surgeon may then use pins or other fixation devices to assist in straightening the toe. These devices may be removed at a later date if necessary. Recovery for hammertoe surgery is approximately 10 to 14 days. You are able to walk immediately following the surgery in a surgical shoe. Swelling may be present but is managed as needed. Physical therapy is used to help reduce swelling in the toe or toes after surgery. Most of these toe surgeries can be performed in the office or the outpatient surgery under local anesthesia.
 Prevention
Prevention Although there is little doubt shoes are responsible for causing corns, the size, shape and other characteristics of our feet are hereditary. A severe bunion may cause a hammertoe, as the great toe twists over or under the second toe, causing it to dislocate.
All The Things You Should Know About Heel Pain
Overview

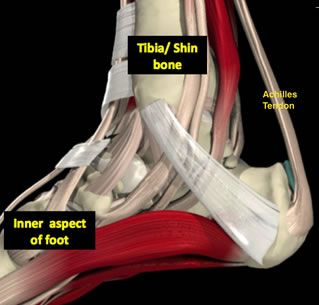
The heel bone is the largest of the 26 bones in the human foot, which also has 33 joints and a network of more than 100 tendons, muscles, and ligaments. Like all bones, it is subject to outside influences that can affect its integrity and its ability to keep us on our feet. Heel Pain, sometimes disabling, can occur in the front, back, or bottom of the heel.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Sever?s Disease. This is a condition that occurs in 10 - 15 year old children, predominantly boys and is associated with running and repetitive jumping. It is also associated with flimsy footwear that kids may wear. It occurs when the Achilles tendon continually pulls on the apophysis of the calcaneum and does not allow for it to fuse with the body of the calcaneum. Calcaneal enthesopathy. This occurs when there is repetitive trauma at the attachment of the Achilles tendon, resulting in a spur from the calcaneum up into the Achilles tendon. It is usually visualized on x-ray and may be tender if there is an associated bursitis or tendonitis. "Pump Bump". Also known as Haglund?s Deformity, this is a bony enlargement that exists on the back of the heel - usually related to a congenital abnormality or with chronic bursitis, causing a thickening. There may have already been trauma or pressure from footwear. Treatment is usually protection of the bump and correct footwear. Associated with a symmetrical swelling at the base of the Achilles tendon. It is usually related to repetitive trauma or inappropriate footwear. It is often red and hot in the early stages. Treatment is usually to correct the footwear, provide padding and treat the local symptoms e.g. ice, rest, physiotherapy and cortisone injection. Fat Pad Syndrome. Direct contact with the base of the heel may result in trauma to the fat pad. Related to obesity, training on hard surfaces, uneven grounds, poor shoes especially overlarge shoes which can cause shearing forces on the heel. These conditions are renowned for taking a long time to recover - usually many months.
Diagnosis
Your GP or podiatrist (a healthcare professional who specialises in foot care) may be able to diagnose the cause of your heel pain by asking about your symptoms and examining your heel and foot. You will usually only need further tests if you have additional symptoms that suggest the cause of your heel pain is not inflammation, such as numbness or a tingling sensation in your foot - this could be a sign of nerve damage in your feet and legs (peripheral neuropathy), your foot feels hot and you have a high temperature (fever) of 38C (100.4F) or above - these could be signs of a bone infection, you have stiffness and swelling in your heel - this could be a sign of arthritis. Possible further tests may include, blood tests, X-rays - where small doses of radiation are used to detect problems with your bones and tissues, a magnetic resonance imaging (MRI) scan or ultrasound scan, which are more detailed scans.
Non Surgical Treatment
Treatment for heel pain usually involves using a combination of techniques, such as stretches and painkillers, to relieve pain and speed up recovery. Most cases of heel pain get better within 12 months. Surgery may be recommended as a last resort if your symptoms don't improve after this time. Only 1 in 20 people with heel pain will need surgery. Whenever possible, rest the affected foot by not walking long distances and standing for long periods. However, you should regularly stretch your feet and calves using exercises such as those described. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can be used to help relieve pain. Some people also find applying an ice pack to the affected heel for 5-10 minutes can help relieve pain and inflammation. However, do not apply an ice pack directly to your skin. Instead, wrap it in a towel. If you do not have an ice pack, you can use a packet of frozen vegetables. Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day. Your GP or podiatrist may advise you to change your footwear. You should avoid wearing flat-soled shoes, because they will not provide your heel with support and could make your heel pain worse. Ideally, you should wear shoes that cushion your heels and provide a good level of support to the arches of your feet. For women wearing high heels, and for men wearing heeled boots or brogues, can provide short- to medium-term pain relief, as they help reduce pressure on the heels. However, these types of shoes may not be suitable in the long term, because they can lead to further episodes of heel pain. Your GP or podiatrist can advise on footwear. Orthoses are insoles that fit inside your shoe to support your foot and help your heel recover. You can buy orthoses off-the-shelf from sports shops and larger pharmacies. Alternatively, your podiatrist should be able to recommend a supplier. If your pain does not respond to treatment and keeps recurring, or if you have an abnormal foot shape or structure, custom-made orthoses are available. These are specifically made to fit the shape of your feet. However, there is currently no evidence to suggest that custom-made orthoses are more effective than those bought off-the-shelf. An alternative to using orthoses is to have your heel strapped with sports strapping (zinc oxide) tape, which helps relieve pressure on your heel. Your GP or podiatrist can teach you how to apply the tape yourself. In some cases, night splints can also be useful. Most people sleep with their toes pointing down, which means tissue inside the heel is squeezed together. Night splints, which look like boots, are designed to keep your toes and feet pointing up while you are asleep. This will stretch both your Achilles tendon and your plantar fascia, which should help speed up your recovery time. Night splints are usually only available from specialist shops and online retailers. Again, your podiatrist should be able to recommend a supplier. If treatment hasn't helped relieve your painful symptoms, your GP may recommend corticosteroid injections. Corticosteroids are a type of medication that have a powerful anti-inflammatory effect. They have to be used sparingly because overuse can cause serious side effects, such as weight gain and high blood pressure (hypertension). As a result, it is usually recommended that no more than three corticosteroid injections are given within a year in any part of the body. Before having a corticosteroid injection, a local anaesthetic may be used to numb your foot so you don't feel any pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Have I Got A Ruptured Achilles Tendon?
Overview

A torn or ruptured Achilles tendon is simply no fun at all. This essential cord of strong, fibrous material attaches the heel bone to the calf muscles and is used in just about every movement, from walking and running to jumping and standing on your tip-toes. It also helps bend the foot downwards at the ankle. As the strongest tendon in the body, the Achilles can withstand a force of about 1,000 pounds. About 7 out of every 100,000 people will suffer from a ruptured Achilles at some point in time, with over 80% of these injuries occurring during a recreational sports activity. Athletes have a 24% chance of tearing their Achilles, but competitive runners have a 40 to 50% chance of Achilles tendon rupture during their lifetime.
Causes
Repeated stress from a variety of causes is often the cause of Achilles tendon injury. The stress may occur from any of the following. Excessive activity or overuse. Flat feet. Poorly fitting or inadequate shoes. Inadequate warm-up or proper conditioning. Jogging or running on hard surfaces. Older recreational athlete. Previous Achilles tendon injury (tendonitis/rupture). Repeated steroid injections. Sudden changes in intensity of exercise. Use of fluoroquinolone antibiotics (especially in children). Trauma to the ankle. Tense calf muscles prior to exercise. Weak calf muscles.
Symptoms
A sudden and severe pain may be felt at the back of the ankle or calf, often described as "being hit by a rock or shot" or "like someone stepped onto the back of my ankle." The sound of a loud pop or snap may be reported. A gap or depression may be felt and seen in the tendon about 2 inches above the heel bone. Initial pain, swelling, and stiffness may be followed by bruising and weakness. The pain may decrease quickly, and smaller tendons may retain the ability to point the toes. Without the Achilles tendon, though, this would be very difficult. Standing on tiptoe and pushing off when walking will be impossible. A complete tear is more common than a partial tear.
Diagnosis
The diagnosis is usually made on the basis of symptoms, the history of the injury and a doctor's examination. The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson's test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected.
Non Surgical Treatment
Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.
Surgical Treatment
While it is possible to treat an Achilles tendon rupture without surgery, this is not ideal since the maximum strength of the muscle and tendon rarely returns. The reason is the ends of the tendon are ruptured in a very irregular manner, almost like the ends of a paint brush. As soon as the tendon ruptures, the calf muscle (gastrocnemius muscle) continues to pull on the tendon and the end of the ruptured tendon pulls back into the leg, which is called retraction. Once the tendon retracts, it is never possible to get sufficient strength back without surgery, because the muscle no longer functions at the correct biomechanical length and is now stretched out. There are patients for whom surgery cannot be performed, in particular, due to existing medical conditions that may add to potential for complications following surgery. For these patients, a specially designed boot that positions the foot correctly and takes the pressure and tension off the muscle and tendon is used. Most importantly, a cast is never used because it causes permanent shrinkage (atrophy) of the calf muscle. The special boot permits pressure on the foot with walking. The boot also has a hinge to permit movement of the ankle. Many studies of Achilles tendon ruptures have shown that this movement of the foot in the boot while walking is ideal for tendon healing. If surgery is not recommended, it is essential to obtain special tests to check that the ends of the tendon are lying next to each other so that healing can occur. The best test to do this is an ultrasound and not an MRI.
What Will Be The Causes And Signs Of An Achilles Tendon Rupture
Overview

A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
Often an Achilles rupture can occur spontaneously without any prodromal symptoms. Unfortunately the first "pop" or "snap" that you experience is your Achilles tendon rupture. Achilles tendon rupture most commonly occurs in the middle-aged male athlete (the weekend warrior who is engaging in a pickup game of basketball, for example). Injury often occurs during recreational sports that require bursts of jumping, pivoting, and running. Most often these are tennis, racquetball, squash, basketball, soccer, softball and badminton. Achilles rupture can happen in the following situations. You make a forceful push-off with your foot while your knee is straightened by the powerful thigh muscles. One example might be starting a foot race or jumping. You suddenly trip or stumble, and your foot is thrust in front to break a fall, forcefully over stretching the tendon. You fall from a significant height. It does appear that previous history of Achilles tendonitis results in a degenerative tendon, which can grow weak and thin with age and lack of use. Then it becomes prone to injury or rupture. Certain illnesses (such as arthritis and diabetes) and medications (such as corticosteroids and some antibiotics) can also increase the risk of rupture.
Symptoms
The most common symptom of Achilles tendonitis is a sudden surge of pain in the heel and back of the ankle at the point of injury which is often described as a snapping sensation in the heel. After the injury has occurred, patients then struggle or find it near impossible to bear any weight on the affected leg. Pain can often be most prominent first thing in the morning after the injury has been rested. Swelling and tenderness is also likely to appear in the area.
Diagnosis
A staggering 20%-30% of Achilles tendon ruptures are missed. Thompson (calf squeeze) test is 96% sensitive and 93% sensitive. Unfortunately, some health practitioners fail to perform this simple clinical test. Ultrasound examination or an MRI can confirm an Achilles tendon rupture.
Non Surgical Treatment
A physical therapist teaches you exercises to help improve movement and strength, and to decrease pain. Use support devices as directed. You may need crutches or a cane for support when you walk. These devices help decrease stress and pressure on your tendon. Your caregiver will tell you how much weight you can put on your leg. Ask for more information about how to use crutches or a cane correctly. Start activity as directed. Your caregiver will tell you when it is okay to walk and play sports. You may not be able to play sports for 6 months or longer. Ask when you can go back to work or school. Do not drive until your caregiver says it is okay.

Surgical Treatment
There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
About
Fashion is in my blood. When I was a kid, my mom would drive me two hours through crazy LA traffic for photo shoots. I used to hang out with the stylists, try on clothes, get advice. It was a great way to grow up. Eventually, I started giving my friends fashion advice, and never looked back.
After 20 years as a stylist for photographers, I was ready to start a business that would let me evolve my own fashion and consulting style. More than anything, I wanted to share my passion for fashion, and watch as my clients discovered the transformative power of a knock-out look.
Today my clients are CEOs, celebrities, corporate and creative people -- men and women who want serious input on their clothing style, advice on what to wear to an event, or how to put together and pack the most versatile travel wardrobe. I also do styling for fashion shoots, including art direction, makeup, hair, clothing and accessorizing. I’ll make you look great. I promise.